Beware of politicians selling “innovative” fixes for problems with obvious solutions.
No one can deny Canadian health care is in crisis: there aren’t enough staff to meet people’s health needs, which is leading to emergency room closures, delayed surgeries, and a shortage of family doctors.
But instead of reinvesting money in an underfunded system, Ontario Premier Doug Ford is aiming to deliver services with for-profit clinics. He describes his approach as “getting creative.”
But Prime Minister Justin Trudeau hasn’t stood up for the Canada Health Act, the federal law that guarantees Canadians access to a publicly funded system. Instead, he has echoed Ford’s rhetoric, suggesting that a “certain amount of innovation should be good.” Meanwhile, former health minister Jane Philpott recently told CBC that the “public-private conversation is a bit of a distraction”—a narrative she’s been pushing in a series of recent interviews.
Whether by right-wing premiers, high-profile pundits, or the Liberal politicians who’ve long claimed to be champions of public health care, the claim of “innovation” is being marshalled not to defend our health care system but to lay the groundwork for its further privatization.

Private delivery of public care is a flaw of our system—not a precedent to build on
People like Philpott advance an insidious argument. They argue that because family doctors technically own their own businesses and some other health care providers operate outside the public system, this shows private delivery of care is not a problem—either in primary care, or in the rest of the system. But there is plenty of evidence that isn’t true. Our system doesn’t work because a lot of health care is delivered privately before being paid with public insurance, but in spite of it.
To take Philpott’s point head on for a moment: allowing family doctors to operate privately instead of being public employees was not a deliberate choice because it was the best way to set up the system; it was a compromise made by Tommy Douglas when he was trying to establish public insurance in Saskatchewan and doctors went on strike to try to stop him. That model then formed the basis for the Canada Health Act, and the system we have today. But it has always had problems.
In a recent interview with PressProgress, health policy researcher Colleen Fuller explained how this model makes it difficult for governments to ensure primary care meets the needs of the public. Since family doctors are businesses, governments can’t tell them where to operate and they’re paid based on an expensive and inefficient fee-for-service model.
Ironically, in that same CBC interview, Philpott said we’ve figured out how to have public schools across the country, now we need to do so for primary care. She doesn’t seem to recognize how private delivery is a major roadblock to achieving that.

Privatization means longer wait times and higher costs
But this problem goes beyond family doctors and deep into the heart of the hospital system. The message we’re getting from political leaders and parts of the media is that allowing more private delivery will cut wait times and improve access, even though the evidence shows us the opposite.
In Australia, two-tier health care was introduced in the 1990s with a similar promise, but research by health economist Stephen Duckett found that areas with more private provision of care actually had longer, not shorter, wait times. His conclusion was that private health care didn’t improve access or cut waits, but it did allow doctors and investors to make more money.
We don’t need to go so far from home for those examples though. An initiative by Manitoba in the 1990s to allow cataract surgeries in private clinics for an additional fee failed. Saskatchewan’s 2010 program to shift some surgeries to private clinics initially cut wait times, before they ballooned again. A later plan for private MRIs also didn’t result in lower wait times.
Meanwhile, British Columbia’s experience with private knee surgeries found they were much more expensive than those done in public hospitals, and didn’t improve return to work times. In short, private health care doesn’t deliver for Canadians — and we know it.
A crisis borne of austerity cuts
How did we get here in the first place?
In the pundit panel on CBC’s The National two weeks ago, columnist Chantal Hébert confidently asserted that “we’ve been throwing money at the system for more than a decade,” only to be in a worse situation than ever. There are obviously problems with health care delivery in Canada—everyone knows that—but acting like funding isn’t part of the problem is disingenuous. As Hébert surely remembers, our public health care system was hit with a sustained period of austerity through the tenures of Brian Mulroney and Jean Chrétien.
In The Chrétien Legacy, Michael J. Prince explains that after the Liberals’ cuts, “1993 levels of federal spending on health care were achieved again only in 2004, following Chrétien’s retirement.”
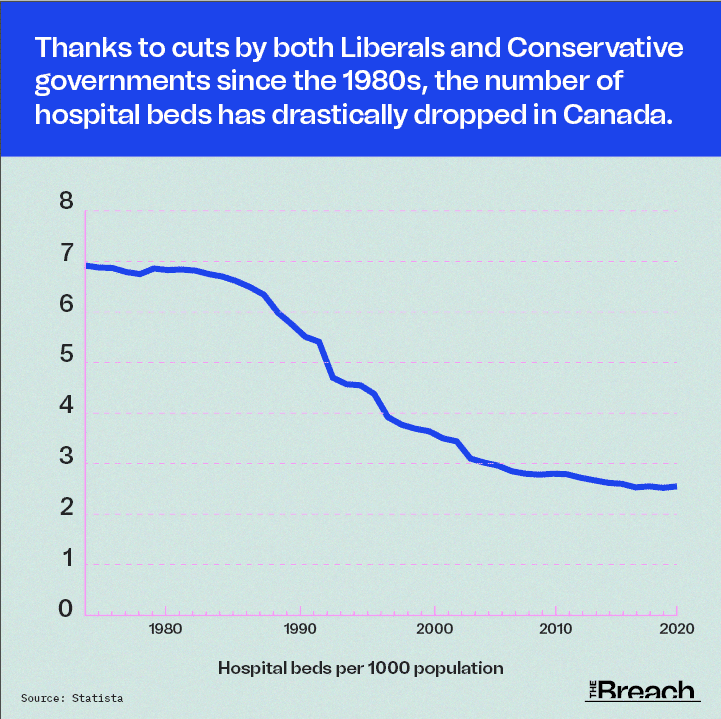
Those cuts had many impacts, from health care staff being laid off to a drastic reduction in hospital beds. Canada had 6.8 hospital beds per 1,000 inhabitants in 1984 when Mulroney took power, but just 2.5 per 1,000 people by 2018. Some of those extra beds would’ve come in handy during the pandemic, not to mention many other high-capacity periods.
We know the problems in our system: they derive from inadequate funding to properly resource our hospitals and expand things like primary care and home care to keep people out of hospital in the first place. But they’re also the product of an overreliance on the private sector throughout the system, even when we know the public system can produce better results if we give it the tools to deliver. That applies to efforts to move surgeries to private clinics, but also more longstanding problems, particularly the lack of universal pharmacare, dental care, and provision of mental health services.
The public remains opposed to privatization
There’s a reason that health care “innovation” and “reform” are always synonymous with increasing private delivery, and it’s not because that results in better care. For decades, we’ve been slowly carving up the public sector—public utilities, key infrastructure, and essential services—and handing it over to private business so they can profit off it. The public health care system has been more insulated from that push, but this crisis offers the private sector an opportunity it won’t pass up without a fight.
Canadians value public health care because they can see the alternative playing out south of the border and don’t want it to return to our country. Even as our public broadcaster gives columnists like Andrew Coyne a national platform to say that the “centre of gravity of public opinion” has shifted to supporting private delivery of care, polling shows the opposite. A new Environics survey found that 59 per cent of Ontarians oppose more involvement by private, for-profit clinics, while 78 per cent say that public money should go to public hospitals and clinics, not the private sector—and that’s in the middle of an unprecedented crisis.
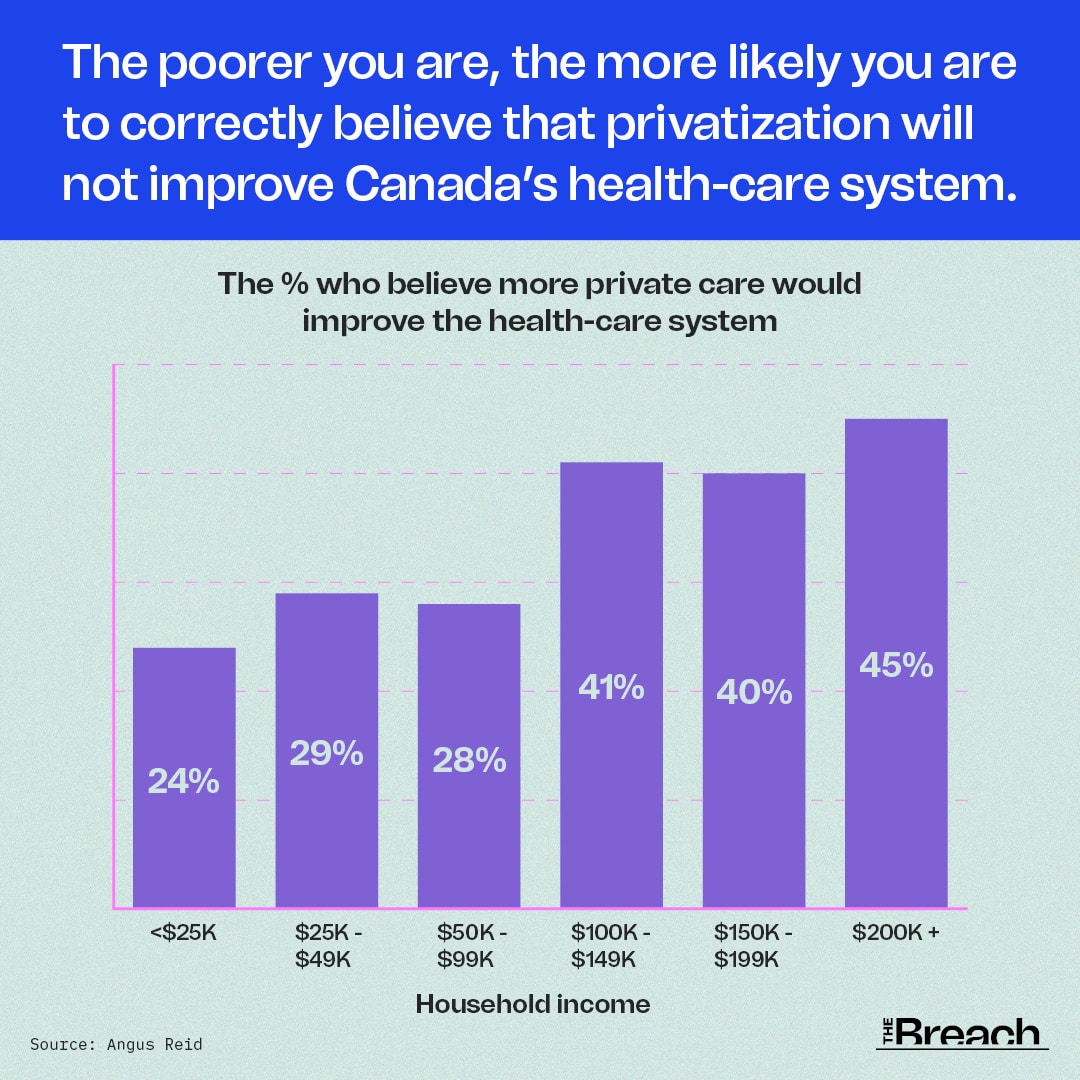
While well-off Canadians, including some in the media brushing off concerns about private delivery, will be able to access high-quality care regardless of whether it’s private or public, the majority of the country knows the same isn’t true for them. They recognize that if we allow the private sector to chip away at our imperfect public system, their access to care and the quality of that care will continue to decline. Only by recommitting to public health care can we get ourselves out of this crisis.

The Breach’s investigations don’t just inform our readers—they force the powerful to react.
An exposé on blood plasma privatization led to national headlines. Our revelations about the government’s cozy connections to Big Pharma sparked a parliamentary probe. A report on high-tech price-fixing by mega landlords resulted in a criminal investigation.
From activists to elected officials, people are using The Breach’s journalism to push for transformative change.
– Dru Oja Jay, Board President, The Breach
Healthcare | How to fix Canada’s healthcare crisis

Privatization | Busting myths about privatized healthcare

Public Health | Conservative provinces exploiting pandemic surgery backlog for privatization assault

1 comment
Comments are closed.
In 1992/3 a federal-provincial-territorial report recommended steep cuts in hospital expenditures – the name of the report was “When Less is Better”. This resulted in the bed cuts referenced in this excellent article. It also triggered layoffs. A 1996 survey of major hospitals across Canada found that 85% had eliminated jobs during the previous two years, resulting in a 10% overall reduction of the hospital workforce. At the same time, the was rising hysteria about the so-called “silver tsunami” of elderly people who were, of course, to blame for the crisis in the health system.